The metabolic cost of plastic
How microplastics and nanoplastics may be quietly reshaping pancreatic function
The pancreas is rarely the first organ people think about in the microplastics conversation. It may also be one of the clearest reminders that environmental exposures do not have to look dramatic to become metabolically important.
Over the past decade, microplastics and nanoplastics have moved from an environmental concern to a biological one. These particles have now been detected in human blood, in vascular plaque, and in pancreatic tumor tissue [1-2,5]. That does not prove they are causing pancreatic disease in people. It does change the starting point. We are no longer asking whether plastic can enter the body. We are asking what those particles may do once they are there.
This paper focuses on that narrower scientific question. It does not argue that microplastics have been proven to cause diabetes in humans. The current human evidence does not support that claim. What the literature does support is a biologically plausible set of mechanisms by which microplastic and nanoplastic exposure could interfere with pancreatic function, insulin signaling, and broader metabolic homeostasis [3-4,6,10,12-13,28]. The aim here is to map those mechanisms carefully, separate animal and in vitro evidence from human evidence, and make clear where the signal is strong, where it is still emerging, and where the field remains uncertain.
Why this topic matters
Metabolic disease now sits at the center of modern public health. Type 2 diabetes, insulin resistance, fatty liver disease, and obesity are usually discussed through diet, physical activity, genetics, sleep, and age. Those factors remain central. But they do not act in isolation. Environmental exposures can shape metabolic vulnerability too, and that idea is already well established for classic endocrine disrupting chemicals such as bisphenol A [9,29].
Microplastics and nanoplastics may represent a newer and more complex version of that problem. They are not simply chemicals. They are also particles. That means they can behave as foreign bodies, as reactive surfaces, and as carriers for additives or co contaminants at the same time [27-28]. They can interact with membranes, mitochondria, immune pathways, and digestive proteins in ways that do not fit neatly into older toxicology categories.
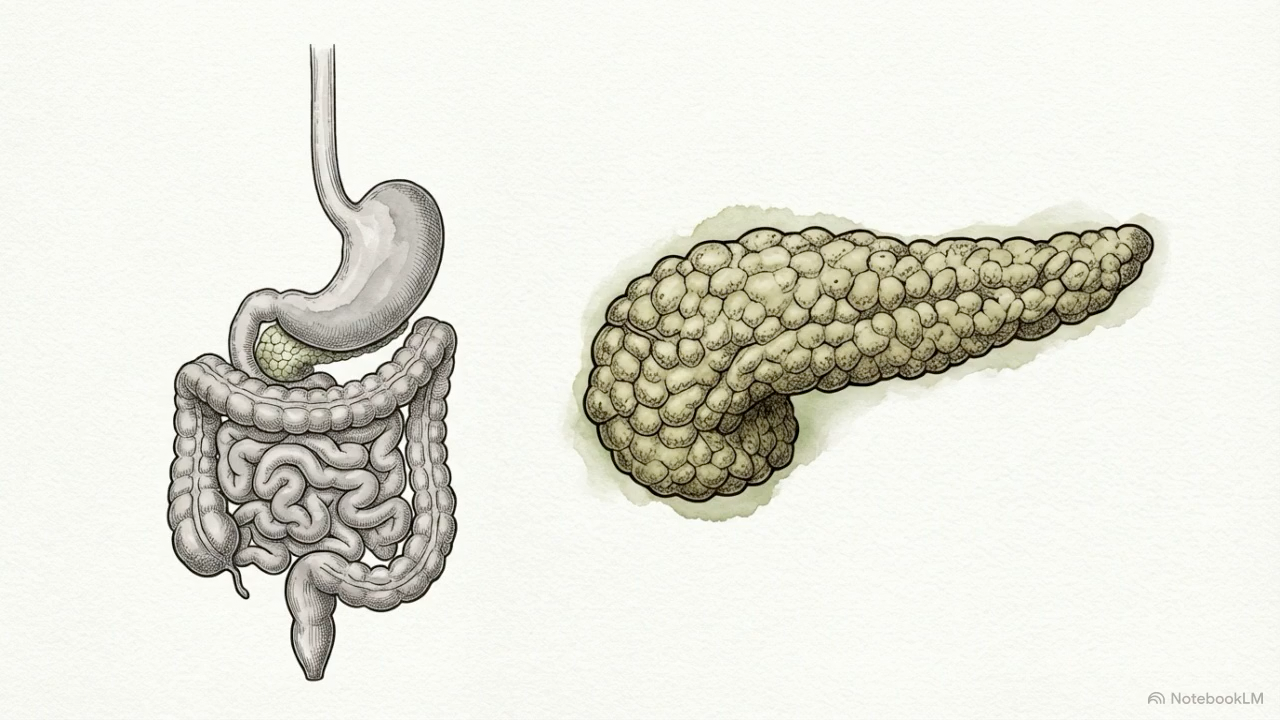
The pancreas is a plausible target for those effects. It is both a digestive organ and a metabolic regulator. Its exocrine compartment produces enzymes that help break down fats, proteins, and carbohydrates. Its endocrine compartment, especially the beta cells within the islets, helps maintain blood glucose through insulin secretion. If either side of that system begins to drift, the effects do not stay neatly contained. Digestion can change. Glucose control can weaken. Insulin resistance can deepen. Over time, the entire metabolic system can become less resilient [6,12,28,31].
Biological background
Microplastics are usually defined as plastic particles smaller than 5 millimeters. Nanoplastics are smaller still, generally below 1 micrometer, with some definitions reserving the term for particles below 100 nanometers. That difference matters biologically. Smaller particles have more surface area relative to their size, interact differently with cells, and are more likely to cross biological barriers or be taken up into tissue [2,27].
The pancreas itself is unusually sensitive to this kind of stress. Its beta cells have high energetic demand and relatively limited antioxidant defenses compared with some other tissues [27-28]. Its exocrine cells are constantly synthesizing and packaging digestive enzymes. Its blood supply places it downstream of intestinal absorption and gut derived inflammatory signals. In practical terms, it sits in a position where it can be exposed both to absorbed particles and to the consequences of gut barrier disruption, dysbiosis, and metabolic endotoxemia [13,24,26,28].
That makes the pancreas a useful place to look. If microplastics are interacting with metabolism in meaningful ways, the pancreas is one of the organs where that signal should appear.
The strongest animal signal begins in pigs
The clearest pancreas centered evidence so far comes from a series of porcine studies using oral PET microplastic exposure. Pigs matter here because their gastrointestinal anatomy, pancreatic structure, and digestive physiology are much closer to humans than those of many rodent models [3-4,15,26].
In the first of these studies, immature pigs exposed orally to PET microplastics for four weeks showed dose dependent pancreatic immune activation and oxidative stress [3]. Transcriptomic analysis identified broad changes in inflammatory signaling, including genes linked to cytokine and chemokine pathways. That matters because it suggests the pancreas is not simply tolerating exposure. It is responding to it.
A follow up metabolomic study showed that the same exposure design altered the biochemical profile of the porcine pancreas [4]. Pancreatic tissue showed changes in glucose, gamma aminobutyric acid, lysophosphatidylcholine, and lysophosphatidylethanolamine, while blood insulin and several serum markers also shifted. These are not disease diagnoses on their own. They are signs that pancreatic metabolism had moved away from baseline after exposure.
The most mechanistically informative pig study came next. In that proteomic analysis, PET exposure altered pathways tied to fatty acid biosynthesis, lipid peroxidation, and digestive enzyme production [15]. Fatty acid synthase activity fell, while free fatty acids rose in pancreatic tissue, especially at the higher dose. Trypsinogen was also altered. That combination points toward oxidative stress, lipid overload, and exocrine dysfunction at the same time.
This is one of the most useful findings in the field because it moves the conversation beyond generic toxicity. The pancreas was not only showing that it had encountered plastic. It was beginning to display a recognizable metabolic stress pattern.
Lipotoxicity as a pancreatic warning sign
One of the most important words in this literature is lipotoxicity.
Lipotoxicity means that fat related molecules begin accumulating in places and at levels where they become harmful rather than adaptive. In pancreatic tissue, that matters because excess free fatty acids can impair both exocrine cells and insulin producing cells. They can also amplify oxidative stress, mitochondrial dysfunction, and inflammatory signaling [15,28].
That is why the porcine PET study is so important. The rise in pancreatic free fatty acids was not just another shifted biomarker. It pointed toward a well recognized mechanism of metabolic injury [15]. In other words, the pancreas was beginning to look less like a stable coordinator of metabolism and more like a tissue absorbing metabolic strain.
This matters clinically because lipotoxic stress is already a familiar feature of insulin resistance and beta cell dysfunction. If plastic exposure contributes to that burden, it may not need to create a completely new disease pathway. It may simply add pressure to one that already exists.
Rodent studies extend the story from tissue stress to glucose dysregulation
Rodent work helps show where these pancreatic changes may lead at the level of the whole organism.
In mice, oral polystyrene exposure has been linked to higher fasting glucose, higher fasting insulin, disturbed gut microbial composition, and weaker hepatic insulin signaling [13]. That study is important because it frames the problem through the gut liver axis rather than through a single organ alone. The pattern it describes is one many metabolic researchers will recognize. Gut disturbance rises first. Inflammatory tone rises next. Insulin signaling becomes less efficient. Glucose handling becomes less stable.
Other mouse studies make the endocrine mechanism more direct. Polystyrene nanoplastics have been shown to induce organ accumulation and insulin resistance in mice [10]. In diabetic mouse models, nanoplastic exposure worsened glucose intolerance, aggravated tissue injury, and deepened insulin resistance [11]. Surface chemistry also changed the metabolic outcome. Amino modified polystyrene nanoplastics produced more severe type 2 diabetes like lesions than pristine or carboxyl modified particles, and the study tied those effects to the Akt and FoxO1 signaling pathway [12]. When that pathway was pharmacologically rescued, the diabetes-like changes were attenuated.
That kind of rescue experiment matters. It means the field is not relying only on loose association. At least in mice, it has identified a specific signaling node through which nanoplastics can worsen metabolic dysfunction.
Microplastics can worsen an already injured pancreas
Another useful question is whether plastics matter only in otherwise healthy systems or whether they can amplify injury in a pancreas that is already under stress.
The answer appears to be yes.
In a mouse model of acute pancreatitis, polystyrene microplastics aggravated pancreatic injury in a dose dependent fashion [17]. They worsened inflammation, increased intestinal barrier disruption, and altered pancreatic proteomic pathways associated with inflammatory and cytoskeletal stress. In a chronic pancreatitis model, oral polystyrene microplastics aggravated disease through reactive oxygen species, NF-κB, TGF-β signaling, and altered gut microbiota [14].
These studies support a second hit model. Microplastics may not need to be sufficient on their own to create overt pancreatic disease in every context. They may still matter if they lower the threshold at which another insult causes more damage.
That framing is useful because it is closer to how chronic disease usually develops in real life. Most people do not become metabolically ill because of one factor alone. Disease emerges when multiple pressures converge.
Oxidative stress is one of the most consistent mechanisms
Across species and models, oxidative stress is one of the most reproducible findings in the microplastic literature [3,7-8,15,18,23,25,27]. It appears in pancreatic tissue, liver tissue, adipose related models, kidney disease models, and broader mechanistic reviews.
In the porcine pancreas studies, PET exposure was associated with oxidative stress signals and impaired antioxidant defenses [3,15]. In duck pancreas, co-exposure to PVC microplastics and cadmium caused mitochondrial damage, reduced ATP production, elevated cytokines, and histological fibrosis [18]. In mouse pancreatitis models, oxidative pathways again sat near the center of the observed injury [14,17].
This matters because pancreatic beta cells are not especially well equipped to tolerate sustained oxidative stress. They have relatively limited antioxidant reserve compared with some other tissues [27-28]. A pancreas repeatedly pushed into oxidative imbalance may become less capable of sustaining normal insulin production, secretion, and recovery after stress.
What remains uncertain is dose relevance. These mechanisms are clear in controlled systems. Whether the same degree of oxidative pressure develops in human pancreatic tissue under ordinary long term exposure remains unproven.
Mitochondrial dysfunction and ER stress add a second layer
Oxidative stress is rarely acting alone. In many systems it is paired with mitochondrial dysfunction and endoplasmic reticulum stress, both of which are highly relevant to pancreatic biology.
A 2022 study found that microplastics together with DEHP synergistically induced pancreatic apoptosis through the GRP78, CHOP, and Bcl-2 related ER stress pathway [6]. That is notable because the endoplasmic reticulum is central to insulin biosynthesis. When beta cells are pushed into chronic ER stress, their ability to fold, process, and secrete insulin can begin to break down [6,28].
Mitochondrial dysfunction points in the same direction. Reviews of environmental nanoplastics consistently describe altered membrane potential, reduced respiratory chain efficiency, increased reactive oxygen species generation, and lower ATP availability [27]. That matters because both digestive enzyme production and insulin secretion are energy intensive processes. A pancreas with less reliable ATP production is a pancreas with less reliable function.
Again, the animal and mechanistic signal is coherent. The open question is how often, and at what exposure burden, this becomes relevant in humans.
Digestion may be affected earlier than blood sugar
The pancreas is not just an insulin organ. It is also a digestive organ. That makes exocrine findings especially important.
In the porcine proteomic study, trypsinogen and other proteins linked to digestive function were altered after PET exposure [15]. That suggests pancreatic disruption may begin at the level of enzyme production, not only at the level of glucose control.
That idea is reinforced by in vitro work showing that polystyrene microplastics and nanoplastics can directly interfere with digestive enzymes. In simulated digestive systems, these particles altered the structure and function of salivary alpha amylase, pepsin, pancreatic protease, and pancreatic alpha amylase [32]. The reported effects included structural destabilization, aggregation, and measurable inhibition of activity.
This does not prove that the same concentrations occur in the human digestive tract during ordinary life. It does show that plastic particles can interfere directly with the protein machinery digestion depends on. For a pancreas centered paper, that is important. It suggests the story may begin earlier than overt blood sugar changes. It may begin with digestion itself.
The gut, the liver, and the pancreas behave like a relay
The pancreas does not work in isolation. It is part of a larger metabolic relay involving the gut, liver, immune system, and microbiome [13,24,26,28].
This is why gut liver axis studies belong in a pancreas paper.
In mice, oral polystyrene exposure has been shown to disturb the gut liver axis in ways that increase the risk of insulin resistance [13]. Inhaled polystyrene nanoplastics have also been reported to induce irreversible hepatic insulin resistance in mice [7]. Low dose polystyrene exposure can increase susceptibility to obesity associated metabolic dysfunction associated steatotic liver disease through gut barrier disruption and microbiota imbalance [24]. Microplastic related changes in the porcine fecal microbiome have been documented as well [26].
What emerges across these studies is a systems picture. Pancreatic dysfunction may not need to begin inside the pancreas. It may begin in the gut, move through the liver, increase inflammatory tone, and only then become visible in pancreatic tissue or glucose dynamics.
That systems framing also helps explain why high fat diet co exposure so often intensifies the plastic signal. The body is already metabolically stressed. Plastic exposure becomes another layer on top of that instability rather than a completely separate event [8,12,23,24].
Broader metabolic models point in the same direction
The pancreatic literature becomes easier to interpret when it is placed beside the broader metabolic literature.
Mixtures of polystyrene microplastics and nanoplastics have been shown to alter fat and glucose metabolism in adipocytes and zebrafish larvae [19]. Polystyrene nanoplastics have been reported to suppress beige fat function and worsen metabolic disorder in high fat diet fed mice [23]. Maternal glucose homeostasis can be disturbed by polystyrene microplastics during pregnancy, and urinary microplastic mixtures have been associated with gestational diabetes risk [20-21].
These studies are not pancreas specific. They matter because they show the same larger pattern. Plastic exposure appears capable of interacting with multiple nodes of metabolic regulation, not just one. The pancreas is part of that network, not an isolated exception.
Human evidence is still early, but it is no longer theoretical
The human evidence needs to be handled with discipline. It is real, but it is not yet sufficient to claim that microplastics cause pancreatic dysfunction or diabetes.
One foundational step came from biomonitoring. Plastic particles have been detected in human blood, showing that at least some fraction of exposure is bioavailable for systemic uptake [2]. Human vascular plaque studies then showed that microplastics and nanoplastics can persist in clinically meaningful tissue, and that their presence was associated with higher cardiovascular event risk during follow up [1]. That is not pancreatic evidence, but it is important context. It proves that human tissue level exposure is not hypothetical.
Human pancreatic tissue evidence has now appeared too. Microplastics have been detected in pancreatic tumor tissue, showing that plastic particles can reach the pancreas in humans [5]. That finding should be interpreted carefully. It does not prove that microplastics cause pancreatic cancer, normal pancreatic dysfunction, or diabetes. It does narrow the translation gap between exposure and organ relevance.
Human metabolic epidemiology is beginning to emerge as well. Higher serum microplastic levels have been reported in insulin treated diabetic patients than in healthy controls, and urinary microplastic mixtures have been associated with gestational diabetes risk [21-22]. These are provocative findings, but they remain observational. They cannot yet distinguish cause from consequence, and they remain vulnerable to confounding and reverse causality.
That is where the field stands today. The human evidence is early, real, and not yet decisive.
Methodological limitations
This field is promising, but it is not tidy.
Most mechanistic studies still use pristine spherical polystyrene, even though real world exposure is more likely to involve weathered, irregular, mixed polymer particles [12,27,28]. That matters because surface chemistry changes biological behavior, and weathering may make some particles more reactive rather than less.
Dose selection is another major challenge. Some experiments use exposures far above estimated daily human intake, while others are closer to environmental relevance [3-4,10,15,28]. Short term animal studies also cannot fully model lifelong, low dose human exposure.
Measurement remains a bottleneck as well. Nanoplastics are especially difficult to detect, quantify, and characterize in biological tissue. Standardization across laboratories is still limited [2,27-28]. Even when particles are measured, it is often unclear whether the observed effects are driven by the polymer itself, its additives, adsorbed contaminants, surface modifications, or some combination of all four [6,12,18,28].
None of these limitations erase the signal. They do shape how confidently that signal can be translated into human risk.
Synthesis
Taken together, the literature now points to a coherent pattern.
In controlled systems, microplastics and nanoplastics can reach metabolic tissues, alter pancreatic gene and protein expression, increase oxidative and inflammatory stress, disturb lipid handling, interfere with digestive enzymes, worsen pancreatic injury, and weaken insulin related signaling [3,4,6,10,12-15,17-18,32]. Those findings have been observed across pigs, mice, ducks, zebrafish, adipocyte models, and human tissue detection studies [3-5,10,12,15-16,18-19].
The most plausible interpretation right now is not that microplastics have already been proven to cause diabetes or pancreatic disease in humans. They have not. The more defensible interpretation is that they increasingly look like metabolism relevant stressors. They may act less like single dramatic causes and more like cumulative burdens that lower the margin of resilience in systems already shaped by diet, inactivity, adiposity, age, and genetic susceptibility [12-13,23-24,28-29].
That is enough to justify serious attention.
Open questions
The next phase of this field is fairly clear. We need more pancreas specific human biomonitoring. We need more studies using weathered and mixed polymer particles. We need better separation of particle effects from leachate and additive effects. We need longer duration, lower dose exposure models that better reflect real world conditions. And we need prospective human studies that connect measured body burden to changes in pancreatic function, insulin sensitivity, and metabolic outcomes over time [21-22,27-28,31].
Those are not academic details. They are the difference between biological plausibility and usable risk characterization.
Conclusion
The pancreas may become one of the more revealing organs in the microplastics story. Not because the evidence is complete, but because the mechanisms are beginning to align.
Oxidative stress appears early [3,14,18]. Mitochondrial dysfunction and ER stress make the signal more specific [6,27]. Lipotoxicity gives that signal a familiar metabolic shape [15]. Exocrine disruption suggests the story may begin before overt glucose abnormalities are even visible [15,32]. Gut liver axis disruption helps explain how local pancreatic changes can be part of a larger metabolic relay [13,24,26]. And early human tissue studies show that exposure has already moved beyond theory [1-2,5,21-22].
The literature does not justify certainty. It does justify attention.
Environmental exposures do not have to look dramatic to become metabolically important. That may be one of the quieter lessons the pancreas is beginning to teach us.
References
- 1.↑ Marfella, R. et al. Microplastics and Nanoplastics in Atheromas and Cardiovascular Events. N. Engl. J. Med. 390, 900–910 (2024). AtlasPubMed
- 2.↑ Leslie, H. A. et al. Discovery and quantification of plastic particle pollution in human blood. Environ. Int. 163, 107199 (2022). PubMed
- 3.↑ Mierzejewski, K. et al. Oral exposure to PET microplastics induces the pancreatic immune response and oxidative stress in immature pigs. BMC Genom. 26, 578 (2025). AtlasPubMed
- 4.↑ Mierzejewski, K. et al. Ingested PET microplastics alter the metabolomic profile of the porcine pancreas. Sci. Rep. 15, 39227 (2025). AtlasPubMed
- 5.↑ Zhao, J., Zhang, H., Shi, L., Jia, Y. & Sheng, H. Detection and quantification of microplastics in various types of human tumor tissues. Ecotoxicol. Environ. Saf. 283, 116818 (2024). AtlasPubMed
- 6.↑ Wang, Y., Zhang, Y., Sun, X., Shi, X. & Xu, S. Microplastics and di (2-ethylhexyl) phthalate synergistically induce apoptosis in mouse pancreas through the GRP78/CHOP/Bcl-2 pathway activated by oxidative stress. Food Chem. Toxicol. 167, 113315 (2022). AtlasPubMed
- 7.↑ Yang, Z. et al. Airborne Nanoplastics Exposure Inducing Irreversible Glucose Increase and Complete Hepatic Insulin Resistance. Environ. Sci. Technol. 58, 3108–3117 (2024). AtlasPubMed
- 8.↑ Okamura, T. et al. Oral Exposure to Polystyrene Microplastics of Mice on a Normal or High-Fat Diet and Intestinal and Metabolic Outcomes. Environ. Heal. Perspect. 131, 027006 (2023). AtlasPubMed
- 9.↑ Alonso-Magdalena, P., Morimoto, S., Ripoll, C., Fuentes, E. & Nadal, A. The Estrogenic Effect of Bisphenol A Disrupts Pancreatic β-Cell Function In Vivo and Induces Insulin Resistance. Environ. Heal. Perspect. 114, 106–112 (2006). PubMed
- 10.↑ Fan, X. et al. Effects of oral administration of polystyrene nanoplastics on plasma glucose metabolism in mice. Chemosphere 288, 132607 (2022). AtlasPubMed
- 11.↑ Wang, Y. et al. The effect and a mechanistic evaluation of polystyrene nanoplastics on a mouse model of type 2 diabetes. Food Chem. Toxicol. 173, 113642 (2023). AtlasPubMed
- 12.↑ Wang, Y. et al. Polystyrene nanoplastics with different functional groups and charges have different impacts on type 2 diabetes. Part. Fibre Toxicol. 21, 21 (2024). AtlasPubMed
- 13.↑ Shi, C. et al. Disturbed Gut-Liver axis indicating oral exposure to polystyrene microplastic potentially increases the risk of insulin resistance. Environ. Int. 164, 107273 (2022). AtlasPubMed
- 14.↑ Li, J. et al. Oral Ingestion of Polystyrene Microplastics Aggravates Chronic Pancreatitis Through ROS Induced NF-κb/TGF-β Signaling Pathway and Alteration of Gut Microbiota. FASEB J. 39, e71223 (2025). AtlasPubMed
- 15.↑ Mierzejewski, K. et al. PET microplastics induce lipotoxicity in the porcine pancreas. BMC Genom. 27, 139 (2026). AtlasPubMed
- 16.↑ Brun, N. R. et al. Polystyrene nanoplastics disrupt glucose metabolism and cortisol levels with a possible link to behavioural changes in larval zebrafish. Commun. Biol. 2, 382 (2019). PubMed
- 17.↑ Zheng, J. et al. Polystyrene microplastics aggravate acute pancreatitis in mice. Toxicology 491, 153513 (2023). AtlasPubMed
- 18.↑ Sun, J. et al. Co-exposure to PVC microplastics and cadmium induces oxidative stress and fibrosis in duck pancreas. Sci. Total Environ. 927, 172395 (2024). AtlasPubMed
- 19.↑ Kim, J. E. et al. Mixtures of polystyrene micro and nanoplastics affects fat and glucose metabolism in 3T3-L1 adipocytes and zebrafish larvae. NanoImpact 37, 100549 (2025). AtlasPubMed
- 20.↑ Zhang, R. et al. Polystyrene microplastics disturb maternal glucose homeostasis and induce adverse pregnancy outcomes. Ecotoxicol. Environ. Saf. 279, 116492 (2024). AtlasPubMed
- 21.↑ Ma, Z. et al. A mixture analysis of urinary microplastic levels and risk of gestational diabetes. Environ. Int. 207, 109928 (2026). AtlasPubMed
- 22.↑ Felek, D., Erkoc, M. F., Yaylacı, M. & Turksoy, V. A. Assessment of Microplastic Exposure in Diabetic Patients Using Insulin. Toxics 13, 926 (2025). AtlasPubMed
- 23.↑ Zhang, L. et al. Polystyrene nanoplastics inhibit beige fat function and exacerbate metabolic disorder in high-fat diet-fed mice. Sci. Total Environ. 918, 170700 (2024). AtlasPubMed
- 24.↑ Wei, G. et al. Low-dose polystyrene microplastics exposure increases susceptibility to obesity-induced MASLD via disrupting intestinal barrier integrity and gut microbiota homeostasis. Ecotoxicol. Environ. Saf. 299, 118310 (2025). AtlasPubMed
- 25.↑ Feng, L. et al. PS-MPs promotes the progression of inflammation and fibrosis in diabetic nephropathy through NLRP3/Caspase-1 and TGF-β1/Smad2/3 signaling pathways. Ecotoxicol. Environ. Saf. 273, 116102 (2024). AtlasPubMed
- 26.↑ Gałęcka, I., Rychlik, A. & Całka, J. Influence of selected dosages of plastic microparticles on the porcine fecal microbiome. Sci. Rep. 15, 1269 (2025). AtlasPubMed
- 27.↑ Liu, H., Li, H., Yao, X., Yan, X. & Peng, R. Environmental nanoplastics induce mitochondrial dysfunction: A review of cellular mechanisms and associated diseases. Environ. Pollut. 382, 126695 (2025). AtlasPubMed
- 28.↑ Shruti, V. C., Kutralam-Muniasamy, G., Pérez-Guevara, F. & Alvarez, R. C. Exploring the micro- and nanoplastics–diabetes nexus: Shattered barriers, toxic links, and methodological horizons. Environ. Pollut. 375, 126319 (2025). AtlasPubMed
- 29.↑ Barbieri, M. et al. Is it time to revise the fighting strategy toward type 2 diabetes? Sex and pollution as new risk factors. Ageing Res. Rev. 99, 102405 (2024). PubMed
- 30. Makwana, B. et al. Marine Microplastic Levels and the Prevalence of Cardiometabolic Diseases in US Coastline Counties. J. Am. Hear. Assoc.: Cardiovasc. Cerebrovasc. Dis. 14, e039891 (2025). AtlasPubMed
- 31.↑ Löhr, J.-M., Vujasinovic, M. & Maisonneuve, P. Risk of Pancreatic Cancer in Inflammatory Pancreatic Diseases. Korean J. Gastroenterol. 85, 280–285 (2025). PubMed
- 32.↑ Azhagesan, A. & Chandrasekaran, N. Exposure of Polystyrene Micro- and Nanoplastics to Simulated Human Digestive Enzymatic Systems: Structural and Functional Implications. ACS Omega 10, 10866–10877 (2025). AtlasPubMed
Sign in to start a discussion.